


1Department of Dermatology and 3Department of Internal Medicine, Seoul National University Hospital, Seoul, and 2Center for Skin Cancer and Adverse Skin Reaction to Chemotherapeutics, Seoul National University Cancer Hospital, Seoul, Republic of Korea
Pruritus is a very common symptom in patients, undergoing targeted anticancer therapy. However, the characteristics of pruritus, according to the targeted anticancer agents, are still unclear. The objective of this study was to determine the characteristics of pruritus, induced by targeted anticancer agents, using a questionnaire-based survey. The survey was administered to cancer patients currently receiving anticancer agents. Medical records were also reviewed. A total of 374 cancer patients completed the survey, of which 108 were treated with the targeted therapy. A total of 205 patients had pruritus, of which 66 were under the targeted therapy. Epidermal growth factor receptor inhibitor (EGFRI) users showed the highest prevalence rate of itching and numeric rating scale score for itching. The 5-D itch score was also highest among users of EGFRIs. In conclusion, patients receiving EGFRIs suffer from severe pruritus frequently. They not only experienced long lasting and intense itching, causing sleep discomfort, but also developed itching at specific body sites.
Key words: chemotherapy; adverse drug reaction; pruritus.
Accepted Jan 23, 2019; E-published Jan 23, 2019
Acta Derm Venereol
Corr: Seong Jin Jo, MD, PhD, Department of Dermatology, Seoul National University Hospital and Center for Skin Cancer and Adverse Skin Reaction to Chemotherapeutics, Seoul National University Cancer Hospital, 101 Daehag-ro, Jongro-gu, Seoul, Korea. E-mail: sj.jo@snu.ac.kr
Pruritus is a common symptom in patients undergoing targeted anticancer therapy. In this study, we aimed to assess the features of pruritus in patients undergoing targeted anticancer. A total of 374 cancer patients completed the survey, of which 108 were treated with targeted therapy. A total of 205 (54.8%) patients had pruritus, of which 66 were under targeted therapy. Epidermal growth factor receptor inhibitor users showed the highest prevalence rate of itching, NRS score for itching and 5-D itch score. This study showed that patients receiving epidermal growth factor inhibitors suffer from pruritus frequently and severely.
Cancer patients, who receive anticancer agents, frequently suffer from various systemic toxicities, such as nausea, mucositis, myelosuppression, and many cutaneous manifestations, including pruritus (1, 2). Pruritus, an unpleasant sensation provoking the desire to scratch, is one of the most common cutaneous symptoms manifested during the anticancer therapy (3). It was reported that around 20–30% of patients, undergoing anticancer treatment, suffer from pruritus (4, 5). In these patients, pruritus could affect not only the quality of life (QoL) but also the clinical outcome of anticancer therapy, as severe pruritus induced by treatments would require dose modification or even discontinuation of the anticancer agents (4, 6).
Recently, targeted anticancer therapies, including small-molecule tyrosine kinase inhibitors (TKIs) and monoclonal antibodies (mAbs), were developed and successfully approved for the treatment of breast, colorectal, lung, and various other cancers (7, 8). In contrast to the classic anticancer chemotherapy that non-specifically damages cancer cells, as well as rapidly proliferating normal cells, the new targeted anticancer agents selectively block signal pathways associated with specific cancer growth and progression, thus successfully reducing systemic adverse events (9). However, targeted anticancer agents frequently induce cutaneous side effects, resulting in clinical problems for oncologists and dermatologists (2, 9). In particular, drug-induced pruritus has been reported to occur more frequently with targeted anticancer agents than non-targeted agents (4, 10, 11).
Some investigators surveyed the incidence of pruritus, during anticancer therapy, by measuring the severity of pruritus based on a visual analogue scale (VAS) or the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE) (11–13). These tools are useful and precise in assessing the severity of pruritus, although they do not include other aspects of the symptom, such as the location and the impact on QoL. Moreover, there is a lack of studies, which focus on the association between the symptom and type of targeted anticancer agents that are classified according to the receptor signalling they target, such as epidermal growth factor receptor (EGFR, also known as ErbB1), vascular endothelial growth factor receptor (VEGFR), human epidermal growth factor receptor 2 (HER2, also known as ErbB2), etc. Each agent has its own mechanism of action, and the clinical aspects of pruritus induced by a certain targeted anticancer agent might be different from that induced by others (11, 14).
In this study, we aimed to assess the features of pruritus in patients undergoing targeted anticancer therapies, according to the types of their target receptors. For the multidimensional aspects of pruritus, we used the 5-D itch scale that evaluated the duration, degree, direction, disability, and distribution of pruritus.
In this cross-sectional study, cancer patients (≥18 years old) were recruited from the general oncology outpatient clinics in Seoul National University Cancer Hospital between February and April 2016. They were actively treated with anticancer drugs at the time of the study. Patients without current anticancer therapy were excluded. We conducted a survey on pruritus and skin dryness among those undergoing anticancer therapy, regardless of previous history of itching. Medical history with regards to anticancer treatment was taken from the review of medical records. The Institutional Review Board of Seoul National University Hospital (IRB No. 1601-058-734) approved the study protocol, and written informed consent was obtained from all participants.
In the questionnaire, the participants were asked about their current anticancer therapy status and skin condition. The survey for the skin condition included a numeric rating scale (NRS) for pruritus, the 5-D itch scale, and the skin dryness evaluation. The 5-D itch scale is a multidimensional measure of the pruritus including duration, degree, direction, disability, and distribution (15). A higher 5-D itch score indicates greater impairment. The body distribution of rash was also checked.
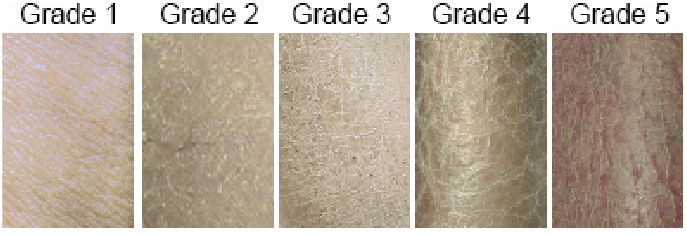
Skin dryness was evaluated by referring to the images, based on the European Group on Efficacy Measurement of Cosmetics and Other Topical Products (EEMCO) guidelines for the assessment of dry skin, then marking the corresponding items (Fig. 1) (16–18).
Fig. 1. The images of skin dryness degree shown to patients for the assessment of dry skin (grade 1 – absent: no scale; grade 2 – mild: faint scaling, faint roughness, and dull appearance; grade 3 – moderate: small scales in combination with a few larger scales, slight roughness, and whitish appearance; grade 4 – severe: small and larger scales uniformly distributed, definite roughness, possibly slight redness, and possibly a few superficial cracks; grade 5 – extreme: dominated by large scales, advanced roughness, redness present, eczematous changes, and cracks).
The following individual clinical information was taken from a retrospective review of the electronic medical records: (i) demographic data (sex, age); (ii) type of cancer (breast, colorectal, haematologic malignancies, lung, stomach, and others); (iii) type of anticancer agents: EGFR inhibitors (EGFRIs, EGFR TKI: erlotinib, gefitinib; Ab: cetuximab; EGFR/HER2 TKI: lapatinib, poziotinib), VEGFR inhibitors (VEGFRIs, TKI: sorafenib, sunitinib; Ab: bevacizumab, ramucirumab), HER2 inhibitors (HER2Is, Ab: pertuzumab, trastuzumab), other target inhibitors (other TIs, atezolizumab, crizotinib, everolimus, imatinib, ipatasertib, rituximab, temsirolimus), and non-targeted agents (adriamycin, carboplatin, capecitabine, cisplatin, cyclophosphamide, docetaxel, etoposide, gemcitabine, irinotecan, navelbine, oxaliplatin, paclitaxel, pemetrexed, vincristine, and 5-fluorouracil); (iv) duration of current anticancer therapy; and (v) radiation therapy history. If two or more different targeted agents are used at the same time, each target is separately counted and coded.
IBM SPSS statistics version 23.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Pearson’s chi-square test, Fisher’s exact test, or the linear-by-linear association method were used to compare the categorical data. Spearman’s rank-order correlation, a nonparametric method, was used for correlation analysis. Nonparametric methods, Mann-Whitney U test or Kruskal-Wallis test, were used for comparing two or multiple groups. Univariate linear regression was performed, in order to find an association between the 5-D itch scale score and skin dryness grade. The differences between variables were considered significant if p-value is < 0.05.
A total of 374 patients, undergoing treatment at Seoul National University Cancer Hospital, were enrolled, including 154 (41.2%) men and 220 (58.8%) women. The mean ± standard error age was 56.50 ± 0.57 years (range 18–84). The mean duration of chemotherapy was 36.82 ± 2.82 weeks (range 1–405). A total of 137 (36.6%) patients received 12 weeks or less, 108 (28.9%) received 13 to 24 weeks, and 129 (34.5%) received more than 25 weeks of anticancer treatment. A total of 99 (26.5%) patients had concomitant or previous history of radiotherapy. The types of cancer were as follows: breast cancer (n = 136, 36.4%), colorectal cancer (n = 113, 30.2%), gastric cancer (n = 33, 8.8%), lung cancer (n = 21, 5.6%), haematologic malignancy (n = 18, 4.8%), and other cancers (n = 53, 1.4%). A total of 322 (86.1%) patients received the first line chemotherapy, while 52 (13.9%) patients received second or third line chemotherapy. A total of 72 (19.3%) patients had a rash. The most common site of the rash was the head (n = 39, 10.4%), followed by the leg (n = 22, 5.9%), arm (n = 20, 5.3%), upper back (n = 19, 5.1%), chest (n = 16, 4.3%), neck (n = 13, 3.5%), shoulder (n = 11, 2.9%), abdomen (n = 11, 2.9%) and lower back (n = 8, 2.1%). Table SI summarizes the demographic and clinical variables as well as the subgroup description according to the type of anticancer agent.
Among the study population, 108 (28.9%) patients were being treated with at least one targeted agent while 266 (71.1%) patients received non-targeted treatment only. The users of EGFRIs, VEGFRIs, HER2Is, and other targeted agents were 23 (6.1%), 34 (9.1%), 31 (8.3%), and 21 (5.6%) patients, respectively. One patient used sunitinib (VEGFRI, platelet-derived growth factor receptor (PDGFR) and c-kit inhibitor) and imatinib (PDGFRI) concurrently.
A total of 205 (54.8%) participants responded that they had pruritus. In addition, 80 (21.4%) answered that they had previous history of itch before chemotherapy. Their mean NRS score was 3.02 ± 0.15 and 5-D itch scale score was 9.46 ± 0.20. Among those with pruritus, 147 (39.3%) were classified as mild (NRS 1 to 3), 44 (11.76%) as moderate (NRS 4 to 6), and 18 (4.8%) as severe (NRS 7 to 10). In terms of skin dryness, 118 (31.6%) responded that they had normal status, while 164 (43.9%) responded mild, 64 (17.1%) – moderate, 25 (6.7%) – severe, and only 3 (0.8%) responded very severe. The scores of NRS, 5-D itch scale, and skin dryness showed a strong correlation (p < 0.001).
There were no significant differences in NRS, 5-D itch scale or skin dryness between groups, stratified by sex and age. According to the duration of chemotherapy divided into the three above-mentioned groups, those undergoing a longer duration of treatment had the tendency to have higher NRS and 5-D itch scale scores (p = 0.026 and 0.013, respectively), but not skin dryness (p = 0.104). In addition, the NRS, 5-D itch scale, and skin dryness were not affected regardless of the patient’s exposure to radiotherapy or whether first line chemotherapy was used or not. Furthermore, patients with rash also showed higher NRS, 5-D itch scale score and skin dryness (p < 0.001, p < 0.001 and p = 0.006, respectively) (Table SII).
Patients with lung (14/21, 66.7%), breast (88/136, 64.7%), and colorectal (62/113, 54.9%) cancer showed a higher prevalence of pruritus than those with haematologic malignancy (7/18, 38.9%) and gastric cancer (11/33, 33.3%). However, the differences in the NRS and 5-D itch scale scores (including each component of the 5-D itch scale) between the different types of cancer were not significant (Fig. 2). Moreover, there was no significant difference in skin dryness between the different types of cancer.
Fig. 2. The scores of the numerical rating scale (NRS, A) and 5-D itch scale (B) among different types of cancer (the bottom and top portion of the boxes represent the first and third quartiles; the band inside the box is the median; the upper and lower whiskers show the highest and lowest results within 1.5 interquartile range of the upper and lower quartile; the square is the mean; the dot is the outlier; the notch means 95% confidence interval of the median).
EGFRI (18/23, 78.3%) and HER2I (23/31, 74.2%) users showed a significantly higher prevalence of pruritus than those receiving non-targeted treatment only (139/266, 52.3%) (p = 0.016 and 0.020, respectively), whereas VEGFRI (19/34, 55.9%) and other TI (6/21, 28.6%) users did not. Subjects with previous history of itching did not show any significant difference according to the types of anticancer agent. Among the patients with pruritus, those treated with EGFRIs (5.28 ± 0.75) and HER2Is (3.22 ± 0.32) showed a significantly higher NRS score than those who received non-targeted therapy only (2.66 ± 0.16) (p = 0.002 and 0.031, respectively). The patients with EGFRIs showed a significant and frequent rash on the head, shoulder, chest, upper/lower back, arm and leg compared to those with non-targeted therapy only. (Table SI) In addition, patients treated with EGFRIs appeared to have a significantly greater 5-D itch score (12.00 ± 0.82) than those who received non-targeted therapy only (9.17 ± 0.24) (p = 0.001) (Fig. 3).
When we examined the details of the 5-D itch scale, patients with pruritus, who used EGFRIs showed significantly higher scores in terms of duration, degree, and sleep than those receiving non-targeted therapy only (p < 0.001, p = 0.001, and p = 0.021, respectively) (Table SIII).
With regards to the distribution score of the 5-D itch scale, patients using EGFRIs showed a significantly higher score than those receiving non-targeted therapy only (p = 0.048) (Table SIII). Remarkably, patients using EGFRIs experienced pruritus more frequently on the face, chest, back, buttocks, and upper arms than those receiving non-targeted therapy only (p = 0.001, p = 0.005, p = 0.032, p = 0.018, and p = 0.045, respectively). Patients using HER2Is had pruritus on the upper arms and forearms more frequently than those receiving non-targeted therapy only (p = 0.016 and p = 0.001) (Fig. 4).
Patients treated with EGFRIs showed a significantly higher grade of skin dryness than those treated with non-targeted therapy only; whereas those treated with VEGFIs, HER2Is, and other TIs did not (Fig. 5). The grade of skin dryness was significantly correlated with the 5-D itch scale as well as the NRS. In particular, skin dryness in EGFRI users showed the strongest association with the 5-D itch scale score (Fig. 6).
Fig. 3. The scores of the NRS (A) and 5-D itch scale (B) among different types of targeted anticancer agents (**p < 0.01, *p < 0.05). (The bottom and top portion of the boxes represent the first and third quartiles; the band inside the box is the median; the upper and lower whiskers show the highest and lowest results within 1.5 interquartile range of the upper and lower quartile; the square is the mean; the dot is the outlier; the notch means 95% CI of the median). EGFRIs: epidermal growth factor receptor inhibitors, HER2Is: human epidermal growth factor receptor 2 inhibitors, Other TIs: other target inhibitors, VEGRIs: vascular endothelial growth factor receptor inhibitors.
Fig. 4. The differences in the positive ratio of itching sites among different types of anticancer agents. The sites were based on the distribution score of the 5-D itch scale. (The cloth represents the ‘point of contact with clothing’ in the 5-D itch scale). EGFRIs: epidermal growth factor receptor inhibitors, HER2Is: human epidermal growth factor receptor 2 inhibitors, Other TIs: other target inhibitors, VEGRIs: vascular endothelial growth factor receptor inhibitors.
Fig. 5. The grades of skin dryness among the different types of anticancer agents. EGFRIs: epidermal growth factor receptor inhibitors, HER2Is: human epidermal growth factor receptor 2 inhibitors, Other TIs: other target inhibitors, VEGRIs: vascular endothelial growth factor receptor inhibitors (***p < 0.001).
Fig. 6. The relationship of the grades of skin dryness and 5-D itch scale score according to the types of anticancer agents. (***p < 0.001, **p < 0.01, *p < 0.05). EGFRIs: epidermal growth factor receptor inhibitors, HER2Is: human epidermal growth factor receptor 2 inhibitors, Other TIs: other target inhibitors, VEGRIs: vascular endothelial growth factor receptor inhibitor.
The recently developed targeted anticancer drugs have achieved high success rates in terms of survival and reduced systemic toxicity (9). Targeted anticancer therapy has paved the way for a new era of anticancer treatment by specifically acting on therapeutic targets or biological pathways with minimal adverse effects on normal tissues (19). However, cutaneous side effects from the novel treatments are increasing (2, 6, 9). Among these treatment methods, EGFRIs show various significant cutaneous toxicities as EGFR is highly expressed on the basal and suprabasal layers of normal keratinocytes and hair follicles (20). EGFRIs eliminate the phosphorylated EGFR in epidermal cells and cause growth arrest and premature differentiation of basal keratinocyte, leading to disturbance of skin barrier function that results in pruritus and skin dryness (20, 21). VEGFRIs, including multiple kinase inhibitors such as sorafenib and sunitinib, could block angiogenesis and disrupt vascular repair mechanism (22). This mechanism frequently causes the hand-foot skin reaction during sorafenib or sunitinib treatment (23). HER2 is a member of the EGFR family, although HER2Is show a lower prevalence of skin toxicity compared to EGFRIs, due to the EGFR dimerization status (24, 25).
Previous studies have reported a higher frequency of pruritus with the use of targeted therapy. In a study of 283 cancer patients, the prevalence rate of pruritus in targeted therapies (35.6%) was higher than in non-targeted therapy only (8.3%) (4). A meta-analysis report showed an incidence rate of 17.4% for all-grade and 1.4% for high-grade pruritus in patients treated with targeted drugs (14). Other meta-analysis studies, including only phase III trials, reported that the relative risk of developing all-grade and high-grade itching with the use of targeted agents compared to controls (including placebo or classical chemotherapy) was 2.19 and 2.56, respectively (11). The risk of pruritus development in targeted anticancer therapy depends on the types of therapeutic target; the prevalence rate of pruritus was reported to be 11.8–33.4% in EGFRIs (11, 14). On the other hand, the reported incidence rate of pruritus for VEGFRIs and HER2Is was 14.0% and 11.2%, respectively (26, 27). In this study, the proportion of patients with itching during chemotherapy was higher than in previous studies, due to inclusion of patients with previous history of itching. This suggested that patients who receive chemotherapy in clinical practice frequently experience itching.
Pruritus could be measured and evaluated by diverse assessment tools (28). The most commonly used measurements are the VAS, NRS, or verbal rating scale (VRS). They can be evaluated easily, but only assess the unidimensional aspect of pruritus. To overcome the limitations of VRS and NRS, several multidimensional methods were developed, which have the advantage of reflecting many of the everyday life problems caused by itching (15, 28–30). Among these methods, authors prefer the 5-D itch scale, as its use is verified in various diseases, associated with pruritus, it is easily completed by participants and includes several problems in everyday life such as sleep, leisure, housework, and employment (31–34).
In our study, patients, who used EGFRIs, showed significantly higher scores both in the NRS and 5-D itch scale than those treated with non-targeted agents, which is consistent with the findings from previous studies (11, 14). The 5-D itch scale score in this group was comparable to that of previous studies on itching diseases (15). In detail, the scores of duration, degree, and sleep (in disability) were significantly higher, implying that EGFRI users suffered a mild to moderate degree of itching 6–12 h a day, with occasional delays in falling asleep. Previous studies showed that in the disability domain of the 5-D itch scale, the sleep item is the most prominent problem (15, 33, 34). With regard to the distribution of itching sites, itching was more common on the face, chest, back, buttocks, and upper arm in the EGFRI group than in the non-targeted therapy only group, which was distinct from the other targeted agents group. Interestingly, a common cutaneous toxicity related to the EGFRI use – papulopustular rash – was frequently noted on the face, trunk, and arms (9, 35, 36). The identical site of pruritus and papulopustular rash occurrence suggests that papulopustular rash is a major skin condition accompanying pruritus in patients using EGFRIs (37, 38). Recent studies suggested that mast cells in papulopustular rash play a pivotal role in EGFRI-induced pruritus (39, 40). Our results also support the necessity of the early and proper management of papulopustular rash to prevent pruritus.
Skin dryness, or xerosis, is another common skin problem in patients receiving targeted anticancer therapies (41). EGFRIs are the most common cause of skin dryness in patients treated with targeted agents (9, 36, 41). EGFR is reported to have a role in epidermal barrier integrity and keratinocyte differentiation (20, 42); EGFR knock-out mice showed dry and flaky skin during development (43). In this study, the EGFRI group showed not only the highest prevalence and severity of xerosis but also the strongest correlation between the skin dryness grade and the 5-D itch scale score among the targeted therapy groups. Similar to previous studies, this finding suggests that skin dryness in patients under the EGFRI treatment is closely related to itching (6, 9, 44).
The pruritus in patients undergoing other targeted therapies showed particular characteristics that are different from those in patients receiving EGFRIs. The HER2I group had a significantly higher prevalence and NRS score of itching compared to the non-targeted therapy only group, although there was no significant difference in the 5-D itch scale score. Remarkably, pruritus was mainly confined to the upper extremities. Previous articles reported that mastectomy could cause abnormal symptoms in the ipsilateral arm (45, 46). As HER2Is are principally administered to a more advanced-stage breast cancer, by insurance coverage protocols in Korea, the findings of the present study could be affected by the radical mastectomy rather than HER2Is itself. VEGFRIs did not show any significant influence in the occurrence of pruritus, in accordance with previous reports (14, 27). Other studies showed a high frequency of itching caused by mTOR (mammalian target of rapamycin) inhibitors or mAb against CTLA4 (cytotoxic T-lymphocyte-associated protein 4) (14). In the present study, only one patient was treated with temsirolimus, who developed itching with a high NRS and 5-D itch scale score and skin dryness grade (7, 13, and 3, respectively).
This study had some limitations. The patients were recruited in a single centre within a limited time period of cross-sectional design. Biomarkers for itching, such as IgE (immunoglobulin E), were not included. The cancer types were largely skewed to breast and rectal cancers, and the targeted agents were not analysed using a single formula due to a small sample size. In addition, the criteria for pruritus and xerosis in the present study were different from that of the CTCAE, which restricted its direct comparison to previous studies.
Patients undergoing targeted anticancer therapy suffer from pruritus frequently and severely. In particular, patients treated with EGFRI experienced long-lasting severe pruritus with characteristic distribution, resulting in sleep disturbances. Clinicians, including oncologists and dermatologists, should pay attention to features of pruritus, in accordance with the specific types of targeted anticancer therapy, for its prevention and proper management.
We would like to thank Soo Min Cho for sketching the human body in Figure 4 and Editage (www.editage.co.kr) for English language editing.
The study was approved by the Institutional Review Board of Seoul National University Hospital
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize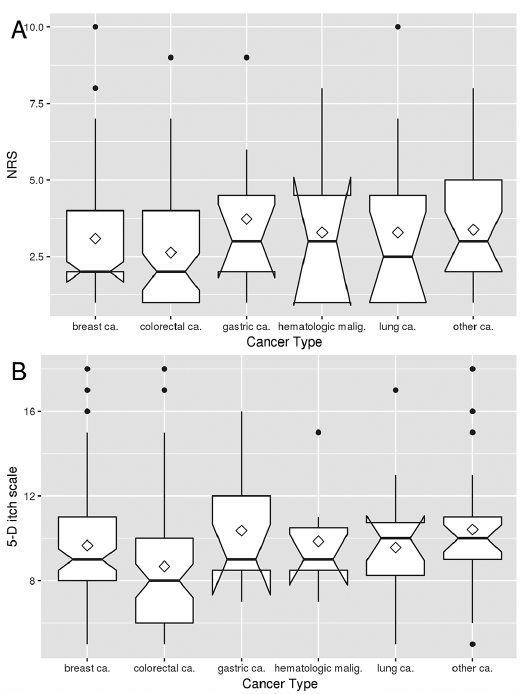 Click to show fullsize
Click to show fullsize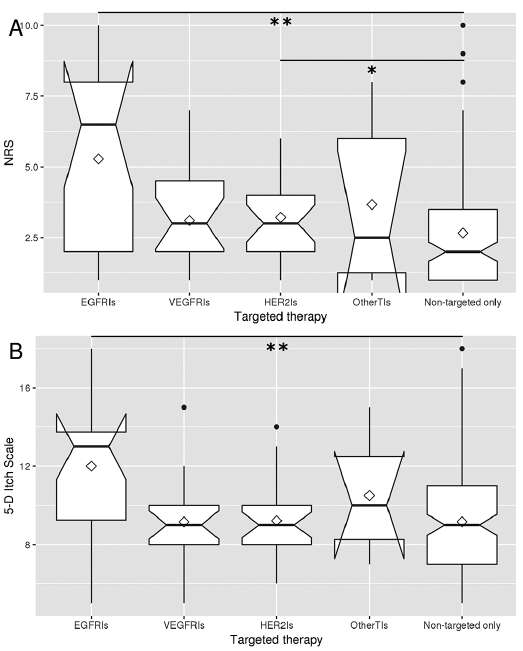 Click to show fullsize
Click to show fullsize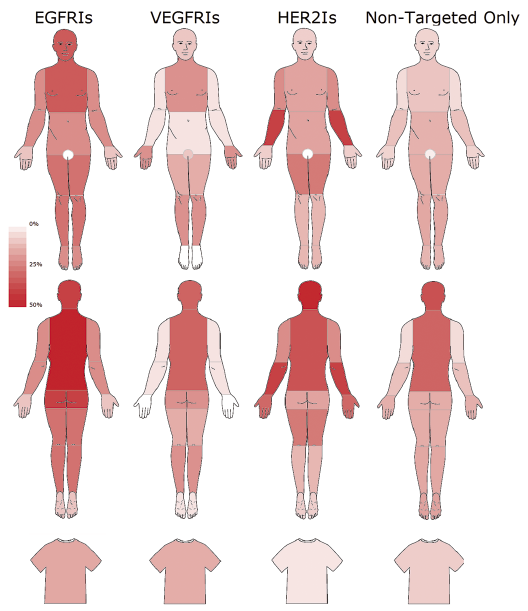 Click to show fullsize
Click to show fullsize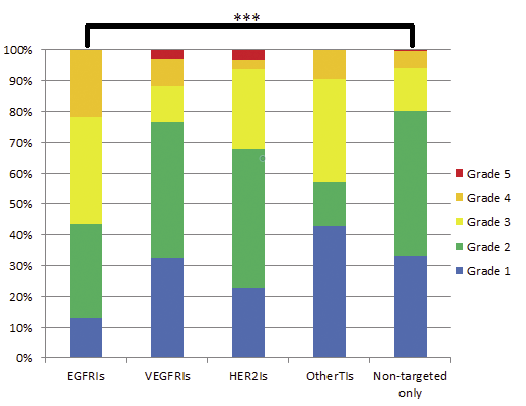 Click to show fullsize
Click to show fullsize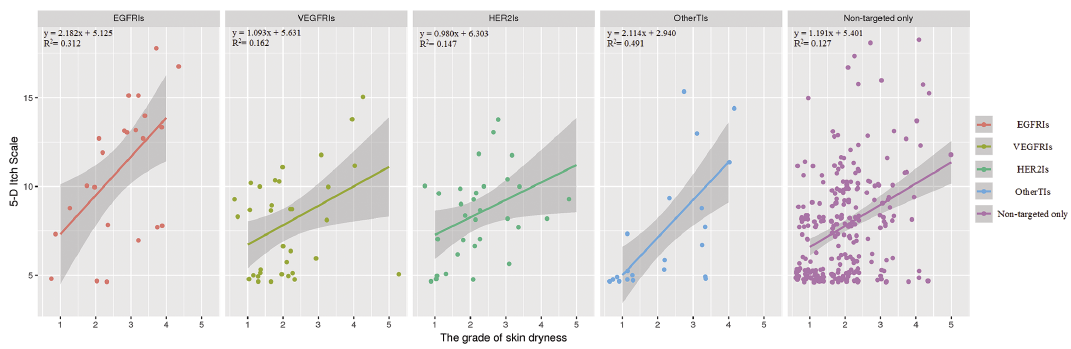 Click to show fullsize
Click to show fullsize